
Evidence of Models Performance
1) It was feasible to engage students in the RHAP (Reducing HIV and AIDS through Prevention) program which used hip-hop/rap music as a method of teaching student about HIV and AIDS awareness and prevention. There were four main constructs used in classroom discussions and in the analysis of music:
This exercise was viewed as educational by the students, as well as one in which they learned about HIV/AIDS. The goal of this program involved causing the students to be more aware of what they listened to and understand that the lyrics may be antithetical to tenets of HIV prevention. Some students stated that, as a result of their participation in this program, they have become more aware of the content of the music and how it relates to behaviors that increase the risk of HIV/AIDS (1).
Since this was a preliminary evaluation of the RHAP program, there were limitations. The program was not tested against other methods of HIV/AIDS education nor was the long-term impact of this program in terms of future sexual behavior assessed. It is also not known whether students who participate in this program will be less likely to engage in risky behaviors such as early initiation of sexual behavior, use of condoms, or avoidance of drugs and alcohol (1).
2) Experiments were put into place with the Management of Organizational Performance, which included induction of self-aiding and self-hindering belief systems. Personal conception of one's own ability can determine motivation, performance and accomplishments when placed in an environment that requires decision-making. People take cognitive ability as either an acquired skill, or something that comes naturally. For those that believe it is an acquired skill, they can set goals and use gaining knowledge in that area as a tool to move forward. They learn what its like to inquire learning goals. Their self-efficacy is strong, they believe in taking up new challenges in order to gain more knowledge, and they aren't afraid of making mistakes,. Rather, it is seen as something that happens naturally, something that is part of the process of learning. They do not necessarily compare their progress to others, but to their own personal and internal standards. (2)
For those that believed their cognitive ability was something that was a fixed capacity were more likely to compare their own ability to others, effecting them socially and in setting performance goals. They can view their own cognitive ability as an intellectual aptitude, thus believing any error or mistake can be an evaluative threat, personally and socially. They prefer to take on tasks that will highlight their own intellectual capabilities and that minimize errors. To them, learning a new task can pose as a threat if it is beyond personal capabilities, and instead of seeing the challenge as a way to grow, it is seen as compromising to their cognitive ability.
Two groups of business school graduates were used in this experiment, the first group was told that cognitive ability was an acquired skill. Their productivity level was high, their self-efficacy was strong and they were motivated in taking on new challenges. Even thought they were designated to difficult tasks, they stayed focused on setting organizational goals and used analytic strategies that allowed them to set their decision rules. (2)
The second group was told that their cognitive theory was inherent, and their productivity was remarkably lower than the first group, their mindsets on their own self-efficacy was lowered and they expressed doubts about their own performance in organizational management. Instead of staying strong and focused on decision making, they become increasingly erratic and unsure of their decisions. (2)
This experiment shows that a person's motivational skills and performances are effected based on their mindset of their own cognitive ability. When a person's self-efficacy is strengthened, their motivation, productivity and performance are heightened, making the individual more confident and willing to achieve more goals. (2)
3) A study on healthcare professionals and their clinical health behaviors was put into place using different social cognitive theories This was an important first step in identifying variables explaining intention and predicting clinical-related behaviors.(3) Studies were conducted in doing research with different literature using data such as information about the authors, the date published, population under study size, design, main theory used, variable predicated (intention/behavior), kind of behavior, and variables measured. (4) Results from the bibliographic screen are presented in Figure 1. Seventy-six studies (N = 20,259 participants) were included in the review. Among these, 16 studies adopted a longitudinal design to predict healthcare professional's behaviors. In addition, 72 of these studies provided information on determinants of intention. (3)
- Expectations (serious and negative consequences of sexually risky behavior such as teen pregnancy and STI’s)
- Observational Learning (risky behaviors described by the artist such as drinking and having sex)
- Reinforcement (the illusion of money and cars as rewards of sexually risky behavior that is often described in the songs)
- Self-efficacy (the illusion of self-efficacy or over confidence that are often described in some songs).
This exercise was viewed as educational by the students, as well as one in which they learned about HIV/AIDS. The goal of this program involved causing the students to be more aware of what they listened to and understand that the lyrics may be antithetical to tenets of HIV prevention. Some students stated that, as a result of their participation in this program, they have become more aware of the content of the music and how it relates to behaviors that increase the risk of HIV/AIDS (1).
Since this was a preliminary evaluation of the RHAP program, there were limitations. The program was not tested against other methods of HIV/AIDS education nor was the long-term impact of this program in terms of future sexual behavior assessed. It is also not known whether students who participate in this program will be less likely to engage in risky behaviors such as early initiation of sexual behavior, use of condoms, or avoidance of drugs and alcohol (1).
2) Experiments were put into place with the Management of Organizational Performance, which included induction of self-aiding and self-hindering belief systems. Personal conception of one's own ability can determine motivation, performance and accomplishments when placed in an environment that requires decision-making. People take cognitive ability as either an acquired skill, or something that comes naturally. For those that believe it is an acquired skill, they can set goals and use gaining knowledge in that area as a tool to move forward. They learn what its like to inquire learning goals. Their self-efficacy is strong, they believe in taking up new challenges in order to gain more knowledge, and they aren't afraid of making mistakes,. Rather, it is seen as something that happens naturally, something that is part of the process of learning. They do not necessarily compare their progress to others, but to their own personal and internal standards. (2)
For those that believed their cognitive ability was something that was a fixed capacity were more likely to compare their own ability to others, effecting them socially and in setting performance goals. They can view their own cognitive ability as an intellectual aptitude, thus believing any error or mistake can be an evaluative threat, personally and socially. They prefer to take on tasks that will highlight their own intellectual capabilities and that minimize errors. To them, learning a new task can pose as a threat if it is beyond personal capabilities, and instead of seeing the challenge as a way to grow, it is seen as compromising to their cognitive ability.
Two groups of business school graduates were used in this experiment, the first group was told that cognitive ability was an acquired skill. Their productivity level was high, their self-efficacy was strong and they were motivated in taking on new challenges. Even thought they were designated to difficult tasks, they stayed focused on setting organizational goals and used analytic strategies that allowed them to set their decision rules. (2)
The second group was told that their cognitive theory was inherent, and their productivity was remarkably lower than the first group, their mindsets on their own self-efficacy was lowered and they expressed doubts about their own performance in organizational management. Instead of staying strong and focused on decision making, they become increasingly erratic and unsure of their decisions. (2)
This experiment shows that a person's motivational skills and performances are effected based on their mindset of their own cognitive ability. When a person's self-efficacy is strengthened, their motivation, productivity and performance are heightened, making the individual more confident and willing to achieve more goals. (2)
3) A study on healthcare professionals and their clinical health behaviors was put into place using different social cognitive theories This was an important first step in identifying variables explaining intention and predicting clinical-related behaviors.(3) Studies were conducted in doing research with different literature using data such as information about the authors, the date published, population under study size, design, main theory used, variable predicated (intention/behavior), kind of behavior, and variables measured. (4) Results from the bibliographic screen are presented in Figure 1. Seventy-six studies (N = 20,259 participants) were included in the review. Among these, 16 studies adopted a longitudinal design to predict healthcare professional's behaviors. In addition, 72 of these studies provided information on determinants of intention. (3)
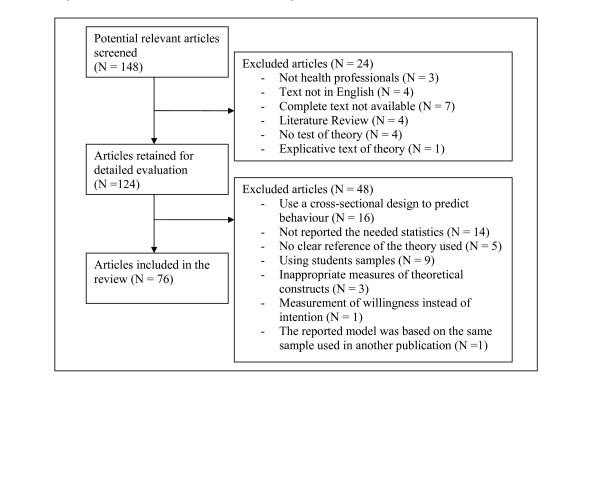
There are a list of limitations that should be taken into account. For one, a limited number of studies predicting behavior were identified. It appears that most of the effort invested was concerned with understanding intention. Not much attention has been given to prospective studies aimed at predicting behavior. More studies on behavior prediction are thus needed to understand which factors explain the cognitive process of decision-making in clinical-related behaviors.(3) Secondly, in the analysis of the efficacy of prediction, there was not a controlled number of variables included in the predictive models. The article acknowledged that this might have inflated the relative performance of some theories over more parsimonious ones.
Unfortunately, only 16 studies were identified, meaning that there must be more studies implemented in order to achieve more accurate information.(3)
4) Evidence in an individuals performance for the Social Cognitive Theory can be seen greatly through self-efficacy and it's effects on health. Efficacy believe is a major source of action. (4) Unless people believe that they can be successful in their actions toward obtaining their goals, they will have little incentive to work towards the goal or even attempt it. In Stanford University's article on the Health Promotion from the Perspective of the Social Cognitive Theory, they state that: " Social cognitive theory views stress reactions in terms of perceived inefficacy to exercise control over threats and taxing environmental demands. If people believe they can deal effectively with potential stressors they are not perturbed by them. But if they believe they cannot control averse events they distress themselves and impair their level of functioning". (4) Most individuals experience stress when learning how to exercise control over environmental demands and when learning how to expand and grow competencies (4). In some cases, low self-efficacy can be detrimental to one's health, at times causing depression, or effecting one's social life. According to the Social Cognitive Theory, there is belief that an individual's efficacy in exercising control over one's health-related behavior can be very effective in their status of health and functioning, thus either strengthening or weakening their performance. (4).
5) Research on self-regulated academic learning has shown that there are multiple components to successful self-regulated learning.
This graph shows the basic series of steps that come with successful self-regulation. According to the article by B. J. Zimmerman, it states that: "Self-Regulated learning strategies are actions and processes that are directed at acquiring information or skills that involve agency, purpose and instrumentally perceptions by learners." (4) Some of these methods include:
- Organizing Information
- Transferring Information
- Self-evaluation
- Self-motivation
- Setting goals
- Meta-cognitive awareness (4)
Social Cognitive theorists believe that self-efficacy is a key factor in affecting self-regulated learners. Research was conducted to support this theory and found that students who had higher self-efficacy had better quality learning strategies verses those who had lower self-efficacy.(4) In Self-Regulated learning, students are able to initiate their own academic skills and accomplish their academic goals without needing to be spurred on by the teacher, a parent or anyone else. Their own motivation is what allows them to succeed academically, thus building their self-efficacy in the SCT. This definition assumes the importance of three perceptions (4)
1) Learning Strategies (4)
2)Perceptions of Performance Skill (4)
3)Commitment to Academic Goals (4)
Sources:
1) Hayden, J. (2009). Introduction to health behavior theory (2nd ed., pp. 173-199). Sudbury, Mass: Jones and Bartlett.
2) Wood, Albert Bandura, R. (n.d.). Social Cognitive Theory of Organizational Management. Retrieved March 28, 2014, from http://www.uky.edu/~eushe2/Bandura/Bandura1989AMR
3)Godin,Bélanger-Gravel, Eccles and JGrimshaw (2008, July 16). Healthcare professionals' intentions and behaviours: A systematic review of studies based on social cognitive theories. Retrieved from http://www.biomedcentral.com/content/pdf/1748-5908-3-36.pdf
4)Stanford University (n.d.). Health Promotion from the Perspective of Social Cognitive Theory. Retrieved April 4, 2014, from http://exordio.qfb.umich.mx/archivos%20pdf%20de%20trabajo%20umsnh/aphilosofia/2007/NEUROPSICOLOGIA/BanHealthPro.pdf
5)Zimmerman, B. J. (1989). A Social Cognitive View of Self-Regulated Academic Learning. Retrieved from http://anitacrawley.net/Articles/ZimmermanSocCog.pdf
1) Hayden, J. (2009). Introduction to health behavior theory (2nd ed., pp. 173-199). Sudbury, Mass: Jones and Bartlett.
2) Wood, Albert Bandura, R. (n.d.). Social Cognitive Theory of Organizational Management. Retrieved March 28, 2014, from http://www.uky.edu/~eushe2/Bandura/Bandura1989AMR
3)Godin,Bélanger-Gravel, Eccles and JGrimshaw (2008, July 16). Healthcare professionals' intentions and behaviours: A systematic review of studies based on social cognitive theories. Retrieved from http://www.biomedcentral.com/content/pdf/1748-5908-3-36.pdf
4)Stanford University (n.d.). Health Promotion from the Perspective of Social Cognitive Theory. Retrieved April 4, 2014, from http://exordio.qfb.umich.mx/archivos%20pdf%20de%20trabajo%20umsnh/aphilosofia/2007/NEUROPSICOLOGIA/BanHealthPro.pdf
5)Zimmerman, B. J. (1989). A Social Cognitive View of Self-Regulated Academic Learning. Retrieved from http://anitacrawley.net/Articles/ZimmermanSocCog.pdf
